CCTV News:According to the message of Wechat WeChat official account of the National CDC, the CDC and the National Health and Wellness Commission have formulated and issued the Prevention and Control Plan for Monkeypox, which proposes to adhere to the principle of "prevention first, combining prevention and control, precise prevention and control, and rapid disposal" and implement the measures of "early detection, early reporting, early isolation and early treatment". The full text is as follows:
Monkeypox prevention and control scheme
Monkeypox is a zoonotic disease caused by Mpox virus (MPXV) infection. In September 2022, China reported the first imported case of monkeypox. Since June 2023, many provinces in China have reported many cases of monkeypox, which leads to a high risk of new local epidemic and hidden transmission. In order to guide all localities to scientifically and accurately do a good job in the prevention and control of monkeypox and effectively safeguard the health of the people, this plan is formulated.
I. General requirements
Adhere to the principle of "prevention first, combination of prevention and control, accurate prevention and control, and rapid disposal" and implement the measures of "early detection, early reporting, early isolation and early treatment". Carry out multi-channel monitoring of medical institutions, key populations, entry personnel and key places. Strengthen epidemic situation analysis and risk judgment, and carry out targeted health education and comprehensive intervention for key populations. Implement measures such as case isolation treatment, epidemiological investigation and follow-up management of close contacts. Insist on finding and controlling together to block the spread of the epidemic in time.
Second, the disease characteristics
(1) Etiological characteristics.
Monkeypox virus belongs to the genus Orthopoxvirus of Poxvirudae, and is a double-stranded DNA virus with a total genome length of about 197kb. The virus was first discovered in monkeys in 1958. In 1970, monkeypox virus was first isolated from a specimen of a suspected smallpox patient in the Democratic Republic of Congo, which was the first confirmed case of human monkeypox.
Monkeypox virus is divided into two evolutionary branches: (1) Branch I, once called Central Africa Branch or Congo Basin Branch; (2) Branch II, once called West Africa Branch, is further divided into IIa and IIb branches. Among them, the strain that caused the outbreak of monkeypox in non-endemic areas of the world in 2022 was IIb branch. At present, there are many subfamilies in IIb, including subfamilies A.1, A.2 and B.1. Since the first imported case of monkeypox was reported in China in September 2022, all the virus sequences submitted to the Institute of Virology of China CDC belong to IIb.
Monkeypox virus is resistant to dryness and low temperature, and can survive for months on the surface of scab skin, soil, clothes, bedding and other objects. The virus is sensitive to heat and can be inactivated by heating to 56℃ for 30 minutes or 60℃ for 10 minutes. 75% ethanol, chlorine-containing disinfectants, peracetic acid and other commonly used disinfectants and ultraviolet rays can effectively inactivate viruses, and are sensitive to hydrogen peroxide, sodium hypochlorite, glutaraldehyde and phthalaldehyde.
(2) Epidemiological characteristics.
1. the source of infection. The host of monkeypox virus is not clear. At present, it is considered that African rodents (African squirrels, tree squirrels, Gambian kangaroos, Dormouse, etc.) may be its natural hosts. Sources of infection include monkeypox cases and infected rodents, monkeys and apes.
2. The route of transmission. Monkeypox virus invades human body mainly through mucous membrane and damaged skin, and is mainly transmitted through direct contact with diseased skin or mucous membrane of the case, or through contact with articles contaminated by virus, inhalation of respiratory droplets of the case for a long time, contact with respiratory secretions, pathological exudates, blood and other body fluids of infected animals, or infection caused by bites and scratches of infected animals.
3. Susceptible population. People are generally susceptible. Vaccination with smallpox vaccine has a certain degree of cross-protection against monkeypox virus.
4. Epidemic characteristics. The epidemic situation of monkeypox before 2021 was mainly endemic in Central Africa and West Africa, and it was mainly spread through contact with infected animals. The transmission chain of human-to-human epidemic was short, mainly sporadic cases and aggregated epidemics of children and young adults, which were occasionally spread to other countries and regions through family or travel. Outbreaks in many countries around the world since May 2022 mainly spread through sexual contact among Men who have sex with men (MSM for short). Most of the cases are young and middle-aged men, which spread through large-scale parties and subsequent MSM in communities and spread to many countries and regions around the world.
(3) Clinical features.
1. incubation period: 5-21 days, mostly 6-13 days.
2. Infectious period: it is contagious after the symptoms appear in the case until the rash and scab naturally fall off and form new skin. Some investigations suggest that some cases may be contagious 1-4 days before symptoms appear.
3. Early symptoms: fever, headache, backache, myalgia and lymphadenopathy may occur.
4. Rash and mucosal rash: usually appear after the fever subsides, and some cases can appear before systemic symptoms. The occurrence of rash often goes through several stages: macula, papule, blister, pustule, scabbing and scabbing. Different forms of rash can coexist, accompanied by obvious itching and pain. It can involve oral and pharyngeal mucosa, anus, genitals, conjunctiva and cornea. Erythema, pigmentation or even scar can be left after scab peeling, and the scar can last for several years.
5. Course and severity. The course of monkeypox is about 2-mdash; 4 weeks, the course of disease of immunocompromised patients may be longer. Monkeypox is a self-limited disease, most cases will disappear on their own, and there are also severe cases and deaths, mainly for children, pregnant women and immunocompromised people.
In the outbreak of monkeypox in many countries around the world since 2022, most cases have mild clinical manifestations, and some cases have no systemic symptoms. The rash is limited to genital and anorectal mucosa, and the deaths are mainly people with low immunity such as untreated HIV-infected people. Since 2022, the mortality rate of cases in non-endemic areas around the world is about 0.1%.
Iii. Publicity, education and intervention
Carry out publicity and education for different groups such as key groups, entry-exit personnel and the general population, strengthen the self-prevention awareness and personal protective measures of different groups in a targeted manner, and actively cooperate with the prevention and control work.
(1) Key groups. Local health and disease control departments, in conjunction with relevant social organizations, fully draw lessons from the comprehensive intervention experience and service model of AIDS prevention and control, and carry out peer education in key activity places such as bars, clubs and baths frequented by MSM. With the help of the mass media, MSM social networking sites and other Internet platforms, we will carry out publicity and education on the prevention and control of monkeypox, raise the awareness of prevention among key groups, reduce high-risk behaviors, guide people with suspicious contact history to consciously do self-health monitoring and enhance their awareness of active medical treatment.
For the requirements of publicity and intervention for key groups, please refer to Annex 1 "Guidelines for Publicity and Intervention for Key Groups".
(2) Entry-exit personnel. Through the distribution of publicity materials and other forms, strengthen the publicity and education of monkey pox prevention and control knowledge for entry-exit personnel. Remind the outbound personnel to pay attention to the information of monkeypox epidemic situation in the destination countries and regions, and not to contact with monkeypox-like symptoms, rodents, primates and other animals. Remind people from countries and regions reporting the epidemic situation of monkeypox that if they have a history of suspicious contact abroad, they should do a good job of self-health monitoring within 21 days after entering the country to avoid close contact with others. In case of monkeypox-like symptoms such as fever, rash and lymphadenopathy, they should take the initiative to see a doctor and truthfully report the epidemiological history.
(3) The general population. All localities give full play to the role of new media and traditional media such as radio, television and newspapers, carry out publicity and education on the prevention and control of monkeypox, and raise public awareness of scientific prevention.
Iv. epidemic monitoring and reporting
(1) Definition of monitoring cases.
1. Monkeypox-like symptoms. Unexplained acute rash (facial or oral mucosa, limbs, genitals or perineum, perianal region, etc.) accompanied by fever (> 37.3℃) or lymphadenopathy.
2. Suspected cases. People with monkeypox-like symptoms have any of the following epidemiological history within 21 days before onset: (1) A history of living in the area where monkeypox cases are reported; (2) Have a history of contact with confirmed or suspected cases of monkeypox; (3) having homosexual sex, or having a history of homosexual sex; (4) Have a history of contact with suspicious animals in endemic areas.
3. Confirmed cases. Monkeypox-like symptoms, suspected cases and close contacts, who are tested positive for monkeypox virus nucleic acid or virus isolation in the laboratory.
(2) Multi-channel monitoring.
1. Monitoring of medical institutions. All kinds of medical institutions at all levels should carry out monitoring of monkeypox-like symptoms, especially those in dermatology (STD), anorectal department, AIDS voluntary counseling and testing clinic, etc. Those who find monkeypox-like symptoms should take the initiative to ask about the epidemiological history, record the patient’s current address and contact information, collect samples and send them to disease control institutions for monkeypox nucleic acid detection. Medical institutions with the ability to detect monkeypox virus and the qualification of monkeypox virus experimental activities can also carry out testing.
2. Monitoring of key populations. All kinds of medical institutions and disease control institutions at all levels should take the initiative to ask whether there are monkeypox-like symptoms and their suspicious contact history when carrying out diagnosis and treatment or testing consulting services for MSM and other key populations. If monkeypox-like symptoms and suspected cases are found, samples should be collected in time for monkeypox virus nucleic acid detection.
3. Immigration personnel monitoring. Upon receipt of the declaration of abnormal health related to monkeypox or the entry personnel with monkeypox-like symptoms found by quarantine, the customs shall collect samples and detect nucleic acids in time, and issue a Convenient Card for Medical Treatment, requiring them to see a doctor as soon as possible; For those who are positive for nucleic acid testing, the relevant information will be reported to the disease control institutions in the jurisdiction, and the relevant departments will further investigate and dispose of them.
4. Sewage monitoring in key places. Conditional areas can carry out sewage monitoring in key activity places such as bars, clubs and baths frequented by MSM according to the local epidemic situation.
(3) Case report.
Relevant medical institutions diagnose patients in time according to clinical manifestations, epidemiology and laboratory test results.
Suspected cases and confirmed cases should be reported directly through the monitoring report management module of China Disease Prevention and Control Information System within 24 hours. If the case is imported from abroad, the country or region of origin should be filled in. Medical and health institutions that do not have the conditions for direct online reporting need to report the information of infectious disease report card to local township hospitals, community health service centers or county-level disease control institutions for online reporting within the prescribed time limit, and fax or send the infectious disease report card to the reporting unit. The medical and health institutions responsible for the direct reporting of cases on the Internet should review and revise the case information in a timely manner according to the laboratory test results and the progress of epidemiological investigation.
Counties (cities, districts) have the first confirmed case of monkeypox or two or more confirmed cases with epidemiological correlation, which should be reported through the public health emergency reporting management information system within 2 hours, and the event level should be "ungraded".
V. Disposal of epidemic situation
(1) Case management.
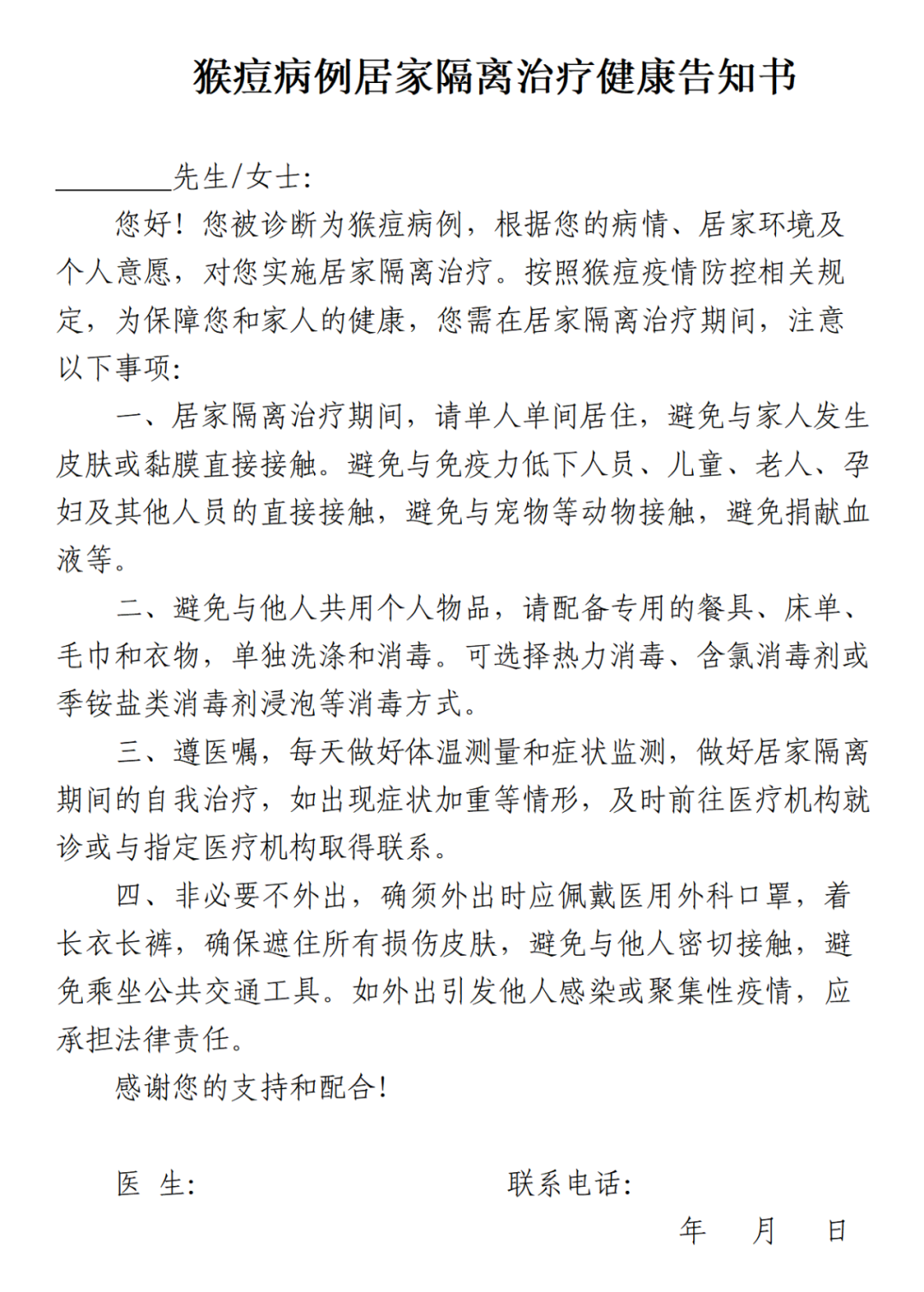
Suspected cases and confirmed cases of monkeypox found around the country should be transported to medical institutions for isolation treatment in time. If the clinical symptoms are obviously improved and the diseased parts have scabbed, they can be turned into home isolation treatment until the rash scabbed naturally falls off and the home isolation is lifted. Confirmed cases with mild illness and conditions of home isolation treatment can be directly treated by home isolation after joint evaluation by medical institutions and disease control institutions. For the confirmed cases of home isolation treatment, the Health Notice of Home Isolation Treatment for Monkeypox Cases will be issued (see Annex 2). During the period of home isolation treatment of confirmed cases, live in a single room, avoid direct contact with family members’ skin or mucosa, disinfect contaminated items, and do not go out unless necessary. When going out, you must wear long trousers and medical surgical masks to avoid going to crowded places and avoiding direct contact with other people’s skin or mucosa. Designated medical institutions arrange special personnel to be responsible for home or telephone follow-up and provide health consultation and medical guidance.
(2) Epidemiological investigation.
County (city, district) level disease control institutions shall, after receiving reports of suspected cases and confirmed cases in their respective jurisdictions, promptly organize epidemiological investigations, find out the source of infection, master, track and manage close contacts, analyze the transmission chain and transmission characteristics, timely discover potential risk groups and their scope and characteristics, and carry out targeted publicity and education and comprehensive intervention. In the process of investigation, give play to the synergy of multi-department joint prevention and control, and obtain comprehensive and accurate flow information as much as possible.
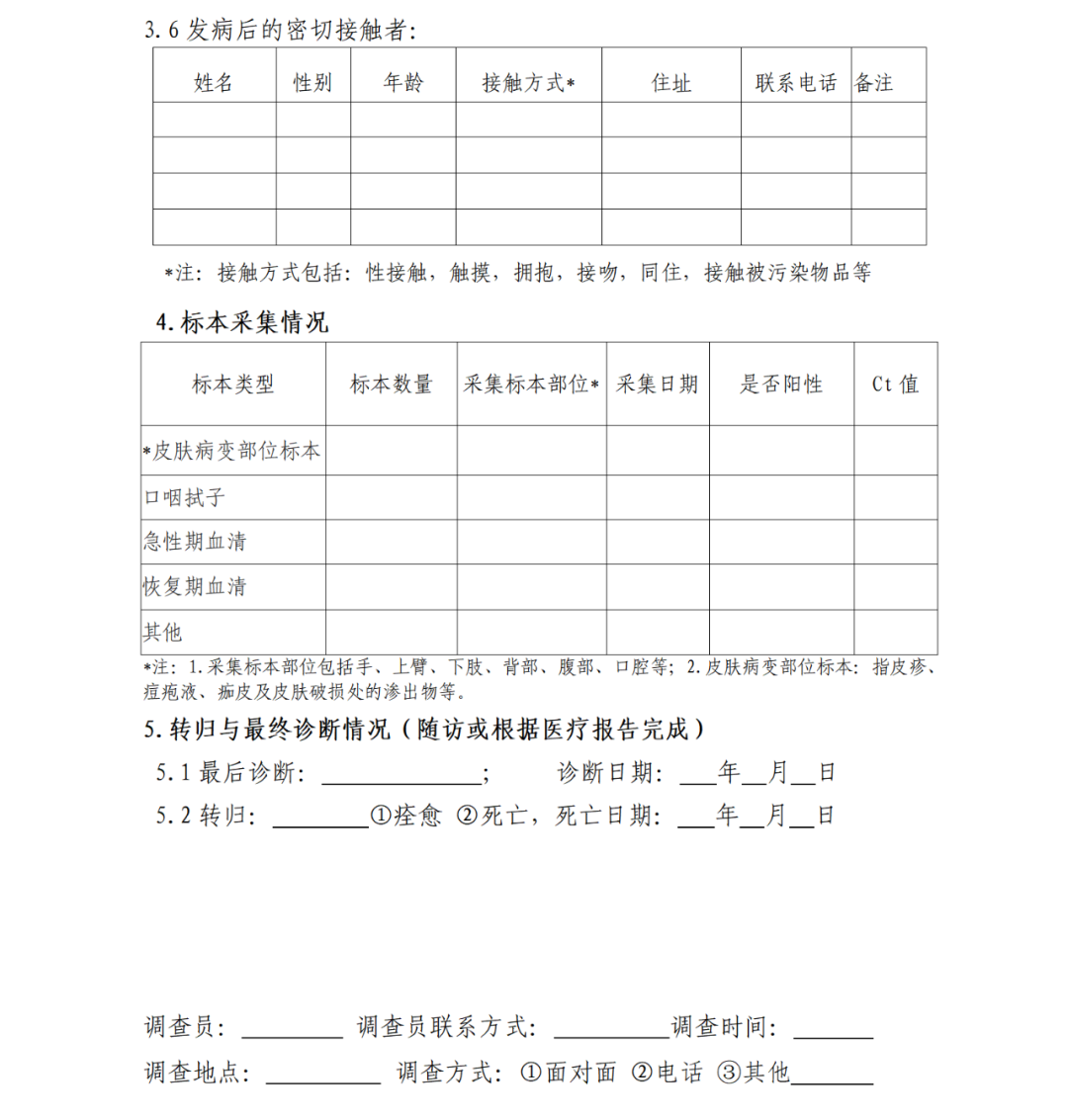
The contents of the investigation mainly include the basic information of the case, the incidence, clinical manifestations, prognosis and laboratory tests; Contact history, contact place and contact mode with suspected infection sources within 21 days before onset; Specific activity places from onset to isolation treatment, people who have direct contact with their skin or mucosa, and those who have sexual contact with them within 4 days before onset.
For the requirements of epidemiological investigation of monkeypox epidemic situation, please refer to Annex 3 "Guidelines for Epidemiological Investigation of Monkeypox Epidemic Situation".
(3) Judgment and management of close contacts.
1. Definition of close contacts. Direct contact with the diseased part of the case and its contaminated items, or infected animals and their secretions, exudates and other pollutants; As well as occupational exposure or long-term close inhalation of respiratory droplets, and those who are assessed to be at risk of infection.
2. Close contact judgment. According to the results of epidemiological investigation and exposure risk assessment, the CDC is responsible for timely judging close contacts.
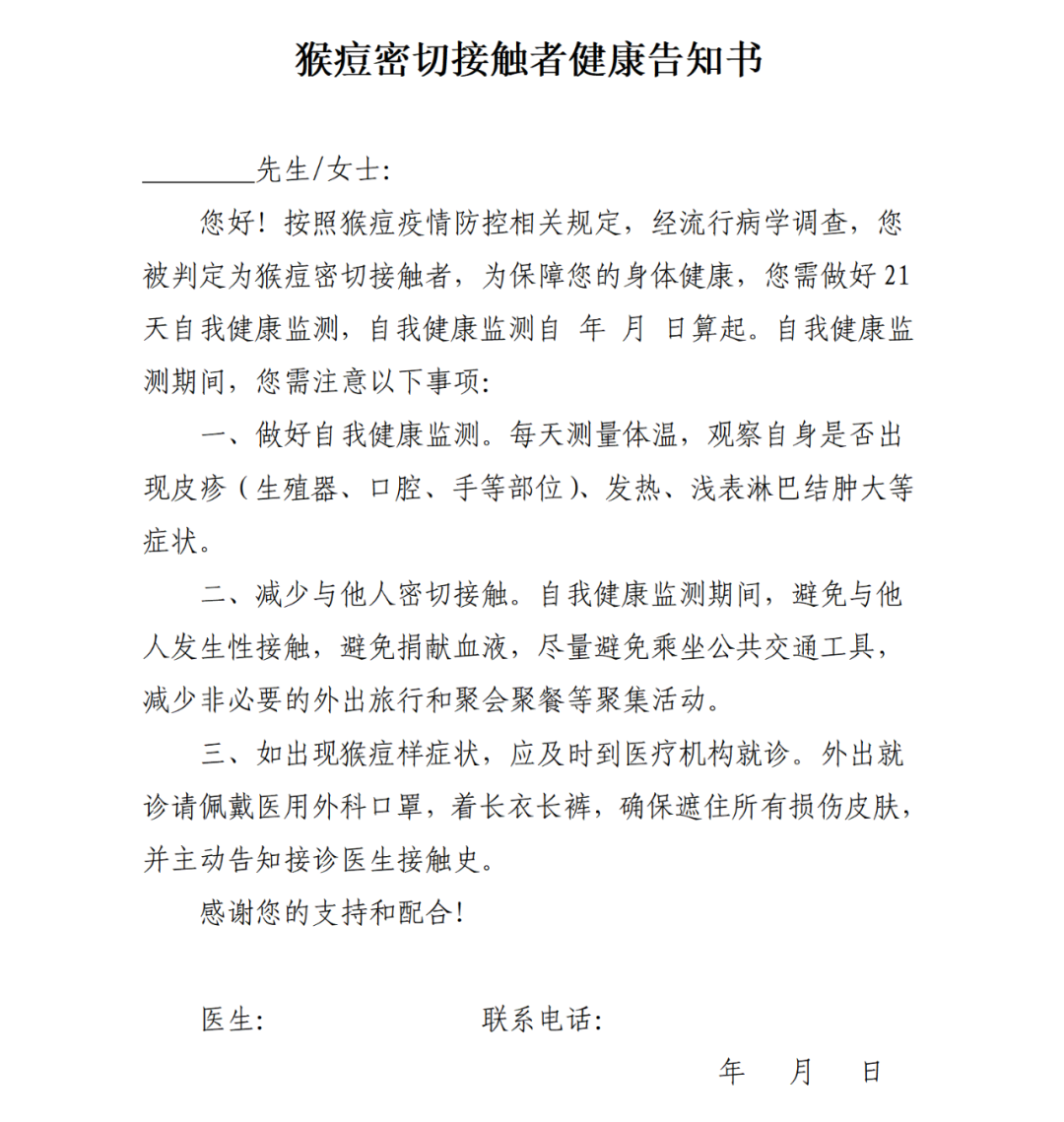
3. Close contact management. Disease control institutions or primary medical and health institutions shall guide close contacts to do self-health monitoring, and the health monitoring period shall be 21 days from the date of the last close contact.
Close contacts can live and work normally during self-health monitoring, and need to avoid close contact with others, such as sexual contact, and avoid donating blood; Insist on daily temperature measurement and symptom monitoring. If you have monkeypox-like symptoms, you should see a doctor in time and report your suspicious contact history. The disease control institutions or primary medical and health institutions in the jurisdiction should follow up the close contacts on the 7th, 14th and 21st days of self-health monitoring, provide consultation and guidance, and handle the abnormal situation in time.
See Appendix 4 "Guidelines for Judgment and Management of Close Contacts of Monkeypox" for the management requirements of close contacts.
(4) Disinfection and personnel protection.
Do a good job in disinfection of personal items such as clothing, towels, sheets and tableware, as well as the environment and surface that may be contaminated by case secretions, exudates and body fluids. Staff engaged in case diagnosis, treatment and nursing, epidemiological investigation, environmental cleaning and disinfection, specimen collection and laboratory testing should do personal protection during their work.
For the disinfection and personnel protection requirements, please refer to Appendix 5 "Technical Guide for Monkey Pox Disinfection" and Appendix 6 "Personal Protection Guide for Monkey Pox".
Six, laboratory testing
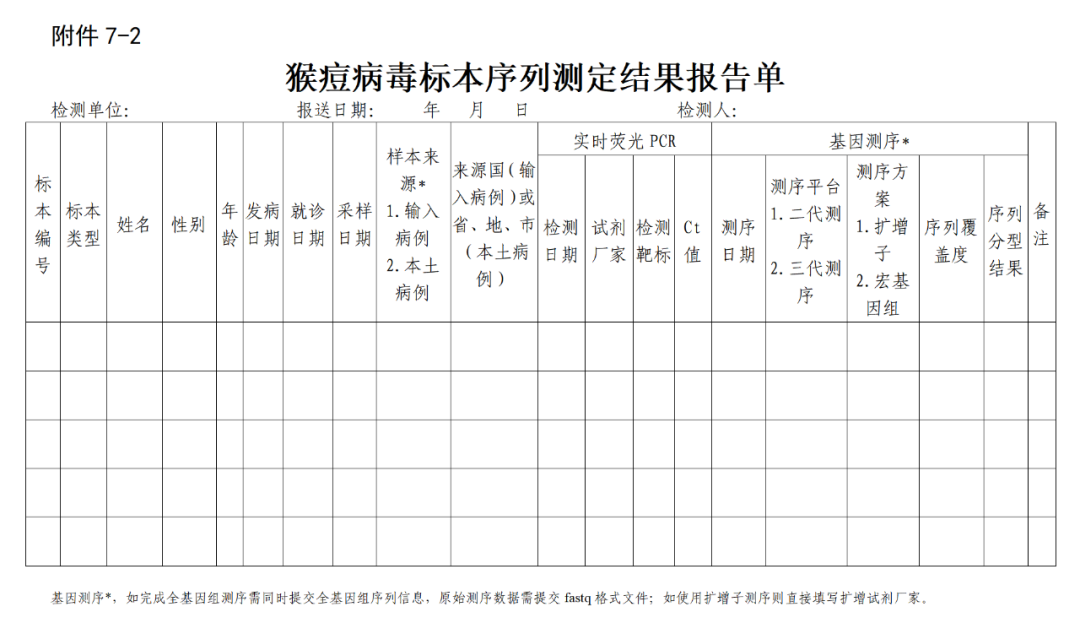
Monkeypox virus nucleic acid detection is the first choice for skin or mucosal lesions, and oropharyngeal swab samples can be collected at the same time. The specimen of the first confirmed case of monkeypox in each province should be sent to the Institute of Virology of China CDC for review; The first or early confirmed cases in local epidemic situation, key confirmed cases with epidemiological correlation with early cases, local confirmed cases with unknown infection source, positive samples of confirmed cases imported from abroad, etc., and the Ct value &le was detected by fluorescence quantitative PCR; The virus gene was sequenced at 32: 00. All original sequencing data, assembly sequences and inspection sheets of sequencing samples shall be submitted to the Institute of Virology, China CDC for summary and analysis within 48 hours after obtaining the sequences. At least one set of samples (including skin or mucosal lesions, oropharyngeal swabs and double sera from patients with positive nucleic acid detection) should be collected from the above confirmed cases and sent to the Institute of Virology, China CDC.
Please refer to Annex 7 "Technical Guide for Laboratory Detection of Monkeypox Virus" for specific requirements of laboratory detection.
Seven, hospital infection control
Medical institutions should strictly control nosocomial infection. Suspected cases and confirmed cases should be placed in isolation wards, and suspected cases should be isolated in single rooms. Medical personnel shall implement standard prevention, adopt isolation and prevention measures for diseases transmitted by contact and droplets, wear disposable latex gloves, masks of KN95/N95 and above, protective face screens or goggles, disposable isolation gown, etc., and do a good job in hand hygiene. In strict accordance with the Technical Specification for Disinfection of Medical Institutions, the body fluids, blood, excreta, secretions, etc. of the cases are treated in a standardized manner, and the medical environment (air, object surface, ground, etc.), medical devices, articles used in cases, etc. are cleaned and disinfected. Do a good job in the disposal and management of medical waste according to the Regulations on the Management of Medical Waste and the Measures for the Management of Medical Waste in Medical and Health Institutions.
VIII. Job Requirements
(1) Strengthen organization and coordination. Local health and disease control departments strengthen close cooperation and information sharing with customs and other relevant departments, timely discover and dispose of the monkey pox epidemic, and implement the work of monkey pox case discovery, epidemic report, diagnosis and treatment isolation, and close contact tracking management to prevent the spread and spread of the epidemic. All localities should pay attention to protecting the privacy of cases, close contacts and key populations during the prevention and control of monkeypox epidemic.
(2) Strengthen publicity and guidance. All localities should timely release relevant information about the monkey pox epidemic in their respective jurisdictions, and do a good job in policy interpretation and public health tips. Through a variety of ways and channels to carry out the publicity of monkeypox prevention and control knowledge, and strengthen the pertinence and effectiveness of publicity and education for key groups. Respond to social concerns in time and guide the public to understand monkeypox scientifically.
(3) Strengthen personnel training. All localities should strengthen the training of professionals in disease control institutions and medical institutions at all levels. Medical staff should be trained in the identification and diagnosis of monkeypox cases, case discovery and reporting, case management and other related knowledge, so as to strengthen the awareness of diagnosis and treatment. Focus on epidemiological investigation, judgment and management of close contacts, laboratory testing, publicity and intervention of key populations and other related knowledge training for disease control personnel to improve the ability of prevention and control of monkeypox epidemic and emergency response.
Attachment:
1. Guidelines for publicity and intervention of key groups
2. Health notification for home isolation treatment of monkeypox cases
3. Guidelines for epidemiological investigation of monkeypox epidemic situation
4. Guidelines for judging and managing close contacts of monkeypox
5. Monkey pox disinfection technical guide
6. Personal protection guide for monkeypox
7. Technical Guide for Laboratory Detection of Monkeypox Virus
Annex 1
Guide to publicity and intervention for key groups
Since May 2022, the epidemic situation of monkeypox in non-endemic areas around the world is dominated by men who have sex with men (MSM). In order to make full use of China’s AIDS prevention and control comprehensive intervention service system, carry out publicity and intervention for key groups such as MSM, prevent the spread of monkeypox epidemic, and form an integrated response mechanism for normalized AIDS and monkeypox comprehensive prevention and control, this guide is formulated.
I. Implementation strategy
On the basis of the existing comprehensive intervention service system for AIDS prevention and control, comprehensive intervention services for monkey pox are provided for the target population from individual, group and society levels through publicity and education, promotion of safe sex, mobilization and testing, outreach services, peer education and Internet intervention.
Second, organize the implementation
Medical institutions and disease control institutions at all levels should strengthen the training of monkeypox knowledge for staff in key departments and AIDS voluntary counseling and testing clinics, and provide services such as publicity of monkeypox prevention and control knowledge, testing consultation and mobilization, treatment and care for key populations. Disease control institutions at all levels should actively promote local MSM volunteers or social organizations with good AIDS prevention and control experience to participate in the publicity work of monkeypox prevention and control, and pay attention to protecting the privacy of key groups in the work process.
Third, the situation analysis
All localities should strengthen the investigation on the epidemic situation, prevention and control status, influencing factors and entry-exit situation of key populations, analyze and judge the epidemic situation of monkeypox in time, and provide a basis for formulating local high-risk behavior intervention work plans. The specific contents include: 1. Key population base, activity form and characteristics, activity place, time and area of entry and exit, etc. 2. Knowledge, attitude and high-risk behavior of monkeypox; 3. The epidemic level of monkeypox and its influencing factors; 4. Monkeypox prevention and control policies and the work carried out by professional institutions; 5. Intervention activities carried out by relevant organizations and individuals, including volunteers; 6. Difficulties and problems affecting the prevention and control of monkeypox.
Fourth, publicity and intervention
(1) Publicity and education. Disease control institutions at all levels or health education professional institutions provide technical support, social organizations participate, jointly study and formulate publicity materials suitable for local characteristics, and strengthen warning publicity and education. Through the mass media, MSM website and dating software based on mobile terminals, the international, domestic and local monkey pox epidemic information and prevention and control knowledge will be publicized to raise the awareness of monkey pox prevention among key populations.
(2) Peer education. Disease control institutions at all levels should strengthen the selection, recruitment and training of peer educators, organize and support peer publicity activities, enhance people’s awareness of monkeypox risk prevention, and promote active testing. Organize regular meetings of peer educators to understand the difficulties and problems in the intervention of monkeypox, and give targeted help and support.
(3) Outreach services. Intervention staff of disease control institutions at all levels regularly go to key population activity places to carry out outreach service activities such as monkey pox publicity, consultation and distribution of publicity materials, improve the awareness and knowledge level of monkey pox prevention of key populations, promote self-health management of key populations, and actively seek testing and consulting services.
(4) Testing consultation. Disease control institutions at all levels mobilize key people with monkeypox-like symptoms or suspicious contact history to carry out monkeypox testing through the Internet, peer education, outreach activities and other forms. Those who find monkeypox-like symptoms in dermatology (STD), anorectum and AIDS voluntary counseling and testing clinics of various medical institutions at all levels should take the initiative to ask about their epidemiological history and sexual contact history, record the patient’s current address and contact information, collect samples and send them to disease control institutions for monkeypox nucleic acid detection. Medical institutions with the ability to detect monkeypox and the qualification for experimental activities of monkeypox virus can also carry out testing. For the areas where the +HIV testing platform in internet plus has been established, the content of monkeypox testing can be increased, so as to realize online testing reservation and result inquiry on the Internet.
V. Intervention in key places
Key venues include physical and virtual venues. Physical venues include bars, clubs, baths and other business venues, while virtual venues include mobile Internet and social media.
(1) Intervention in physical places.
Disease control institutions at all levels are responsible for organizing intervention staff to carry out publicity on prevention and intervention of monkeypox in bars, clubs, baths and other places frequented by local MSM, mainly including:
1. In the bars, clubs, baths and other physical places frequented by MSM, post eye-catching health education publicity pictures and set up health education information bulletin boards;
2. Strengthen personal health responsibility awareness, carry out health consultation on monkeypox, and promote self-risk assessment;
3. Provide referral service information, inform the clear diagnosis and treatment process and related testing, medical institution name, contact person and other information.
All localities should strengthen the intervention and publicity of the places where the confirmed cases of monkeypox have been active within 21 days before the onset of the disease and the places where sewage monitoring is positive, attach importance to the personal privacy protection of the target population, strengthen the training of the prevention and control knowledge of monkeypox for peer educators of social organizations, establish a standardized behavioral intervention process, and improve their self-protection skills.
(2) Intervention in virtual places.
Disease control institutions at all levels are responsible for organizing and guiding the local orderly online publicity of monkeypox, timely publishing and updating the publicity and education content of monkeypox on relevant websites and social media platforms, and forming an online publicity and intervention service system of monkeypox detection-consultation-diagnosis and treatment for key populations.
Disease control institutions at all levels support social organizations or peer educators to organize online consultation and exchange by using websites, mailboxes or social media platforms. Answer all kinds of monkey pox related questions raised by netizens in time. According to the spread characteristics of monkeypox in different periods, experts, professionals and peer educators are regularly or irregularly organized to conduct online education by using the Internet and social media platforms. Disease control institutions at all levels should regularly guide and update relevant professional information to ensure that the publicity content is scientific and effective.
Annex 2
Annex 3
Guide to epidemiological investigation of monkeypox epidemic situation
In order to guide local disease control institutions to standardize the epidemiological investigation of suspected cases, confirmed cases and cluster epidemics of monkeypox, timely grasp the epidemiological information such as case exposure history and contact history, implement the tracking judgment of close contacts, and prevent the spread of the epidemic, this guide is formulated.
I. Purpose of the investigation
(a) to find the source of infection, master, track and manage close contacts.
(2) Analysis of communication chain and communication characteristics.
(three) timely discover the potential risk groups and their characteristics and scope, and carry out targeted publicity and education and comprehensive intervention.
Second, the survey object
Suspected cases, confirmed cases and clustering epidemic.
Third, the survey method and content
By consulting the data, we asked the cases, doctors, family members and insiders for epidemiological investigation. If the condition of the case permits, the case should be investigated first, and then the doctors, family members and insiders should be investigated.
When carrying out case investigation, we should carefully and carefully understand and record the basic information of the case, the incidence of medical treatment, clinical manifestations, prognosis and laboratory testing information; Contact history, contact place and contact mode with suspected infection sources within 21 days before onset; Specific activity places from onset to isolation treatment, people who have direct contact with their skin or mucosa, and those who have sexual contact with them within 4 days before onset.
(1) Basic information. Such as name, gender, age, address, nationality, contact information, etc.
(two) the incidence of medical treatment. Clinical manifestations, laboratory tests, the course of onset and treatment, and the change and prognosis of the disease.
(3) Investigation on the source of infection. Investigate the exposure history within 21 days before the onset of the case, including the travel history or residence history in the reporting area of monkeypox cases at home and abroad, and ask in detail about the contact time, mode, frequency, place and protective measures taken during contact, especially the history of sexual contact. During the investigation, if the contents that are not included in the questionnaire but have important epidemiological significance are found, they should also be inquired and recorded in detail.
(4) Investigation and judgment of close contacts. After tracking and checking the activities and people’s contact during the infection period, determine their close contacts. The judgment and management of close contacts shall be carried out in accordance with the Guidelines for Judgment and Management of Close Contacts of Monkeypox (Annex 4).
For details, please refer to Appendix 3-1 "Monkey pox Case Questionnaire".
Iv. organization and implementation
According to the principle of "territorial management", the county (city, district) level disease control department where the case is located organizes the disease control institutions in the jurisdiction to carry out epidemiological investigation of monkeypox cases, and the medical institutions provide diagnosis and treatment information. The investigation unit shall, according to the investigation plan and purpose, determine the composition of investigators and the division of responsibilities, and carry out case epidemiological investigation in a timely manner. In the process of investigation, give play to the synergy of multi-department joint prevention and control, and obtain comprehensive and accurate flow information as much as possible. During the investigation, investigators should do personal protection.
V. Reporting and analysis of information
After completing the investigation, the CDC should analyze and summarize the cases, timely submit the epidemiological case questionnaire, investigation report and other data to the higher CDC step by step, and keep and archive the investigation data. Case flow information should be in accordance with the relevant provisions, strictly protect information security and personal privacy information.
Attachment: 3-1. Case Questionnaire of Monkeypox Cases



Annex 4
Guide for judging and managing close contacts of monkeypox
This guide is formulated to guide all localities to judge and manage close contacts of monkeypox and effectively control the spread of monkeypox epidemic.
I. Criteria for judging close contacts
Close contact refers to the person who directly contacts the diseased part of the case and its contaminated items, or infects animals and their secretions, exudates and other pollutants; As well as occupational exposure or long-term close inhalation of respiratory droplets, and those who are assessed to be at risk of infection. Specific circumstances include:
1. People who have direct contact with skin or mucosa after the onset of suspected cases or confirmed cases, including sexual contact, touching, hugging and kissing;
2. People who share clothes, bedding, tableware and other items with suspected cases or confirmed cases with rash symptoms;
3. Medical and health workers who may be exposed to viruses during medical treatment, sampling or laboratory testing, and are assessed to be at risk of infection;
4. Persons who have sexual contact with suspected cases or confirmed cases within 4 days before onset, and have been assessed by epidemiological investigation professionals as having the risk of infection, can also be judged as close contacts;
5. People who have been in close contact with suspected cases or confirmed cases for a long time in a narrow confined space (such as living in the same confined space for a long time) can also be judged as close contacts after being assessed by epidemiological investigation professionals as having the risk of infection;
6. Persons who come into contact with animals infected with monkeypox virus and their secretions, exudates and other pollutants without taking effective personal protection;
7. Other persons who may be exposed to the virus.
Second, the management of close contacts
1. Management term and method. The disease control agency at the place where the case is found or the disease control agency at the place where the close contact is located should carry out monkeypox virus nucleic acid detection in time on the day when the close contact is tracked, and inform and guide the close contact to do self-health monitoring, and the health monitoring period is 21 days from the date of the last close contact. During self-health monitoring, you can live and work normally, and you need to avoid close contact with others, such as sexual contact, and avoid donating blood.
2. Informed notification. When implementing health monitoring, the CDC or primary medical and health institutions should verbally inform the reasons, duration, precautions and disease-related knowledge of health monitoring, and be responsible for following up the contacts and contact information of the CDC or primary medical and health institutions, and issue the Health Notice for Close Contacts of Monkeypox.
3. Regular follow-up. Disease control institutions or primary medical and health institutions should take the initiative to inquire about the self-health monitoring of close contacts by telephone or on the 7th, 14th and 21st day, and provide advice and guidance. Found abnormal situation, timely investigation and disposal.
4. Self-health monitoring. Insist on daily temperature measurement and symptom monitoring. The main symptoms include fever (> 37.3℃), rash and superficial lymphadenopathy. Close contacts should go to medical institutions or get in touch with follow-up contacts in time to receive monkeypox virus nucleic acid detection once they have related symptoms.
Attachment: 4-1. Health Notice for Close Contacts of Monkeypox
Annex 5
Technical guide for disinfection of monkeypox
This guide is formulated in order to further standardize the disinfection work related to the epidemic situation of monkeypox, implement scientific disinfection and accurate disinfection, and reduce the harm caused by monkeypox virus to public health.
First, disinfection of epidemic focus
(1) Scope of application.
It is suitable for disinfection at any time and final disinfection of places and articles that may be contaminated after the occurrence of monkeypox cases.
(2) disinfection principle.
1. Determination of scope and objects.
According to the results of epidemiological investigation, the scope and object of field disinfection were determined. Disinfect the environment and articles that may be polluted during the hospitalization and transportation of the case at any time. Disinfect the places where the case lived or moved, such as residence, workplace, study place, diagnosis and treatment place, transport tools, and other places that may be contaminated (such as hospitalization, transfer, discharge and death).
2. Method selection.
(1) Disinfection of medical supplies. Try to choose disposable medical supplies, non-disposable medical supplies should be sterilized by pressure steam first, and heat-labile items can be disinfected or sterilized by chemical disinfectants or low-temperature sterilization equipment.
(2) hand disinfection. It is suggested to use hand disinfectant to rub hands for disinfection, and 75% ethanol, hydrogen peroxide and other disinfectants can also be selected.
(3) Disinfection of environment and object surface. Chlorine-containing disinfectants, chlorine dioxide, peracetic acid, hydrogen peroxide and other disinfectants can be selected for wiping, spraying or soaking disinfection.
(4) Disinfection of textiles such as clothes and sheets. Thermal disinfection, chlorine-containing disinfectant or quaternary ammonium salt disinfectant immersion and other disinfection methods can be selected.
(three) disinfection methods of common pollution objects.
1. Hand disinfection.
Quick-drying hand disinfectant can be selected, or 75% ethanol can be directly used for wiping disinfection; Those who are allergic to alcohol can choose effective non-alcohol hand disinfectants such as quaternary ammonium salts. When there are pollutants visible to the naked eye, you should first use hand sanitizer (or soap) to wash your hands under flowing water according to the six-step washing method, and then disinfect them according to the above method.
2. Skin and mucous membrane.
When the skin is polluted by pollutants, the pollutants should be removed immediately, and then 0.5% iodophor or hydrogen peroxide disinfectant should be dipped with disposable water-absorbing materials for wiping and disinfection for more than 3 minutes, and then cleaned with clean water; Mucosa should be washed with plenty of normal saline or 0.05% iodophor for disinfection.
3. Sheets, towels, clothes and other textiles.
When the textiles such as sheets, towels and clothes used in the case have no visible pollutants, if they need to be reused, they can be disinfected by circulating steam or boiling for 30 minutes; Or soak it in chlorine-containing disinfectant with available chlorine of 500mg/L or quaternary ammonium salt disinfectant of 1000mg/L for 30 minutes, and then clean it as usual; Or use other effective disinfection methods. Clothes that are not resistant to moisture can be disinfected by ethylene oxide or dry heat.
When there are pollutants such as secretions, exudates, excreta, blood, body fluids, etc., it is recommended to treat them centrally as medical wastes.
4. Dining (drinking) utensils.
The tableware (drinking utensils) such as bowls, plates, chopsticks and cups used in the case were boiled and disinfected for 30 minutes, or soaked in chlorine-containing disinfectant with effective chlorine of 500mg/L for 30 minutes, and then washed with clear water.
5. pollutants.
A small amount of pollutants such as case secretions, exudates, excreta, blood and body fluids can be carefully removed with disposable absorbent materials (such as gauze and rags) and chlorine-containing disinfectants (or disinfectant wipes/dry towels that can achieve high-level disinfection) with effective chlorine of 5000-10000mg/L/L..
A large number of pollutants such as case secretions, exudates, excreta, blood and body fluids should be completely covered with disinfectant powder or bleaching powder containing water-absorbing components, or after being completely covered with disposable water-absorbing materials, a sufficient amount of chlorine-containing disinfectant with effective chlorine of 5000-10000mg/L should be poured on the water-absorbing materials for more than 30 minutes (or a disinfection dry towel that can reach a high level of disinfection) and carefully removed. Avoid contact with pollutants during the cleaning process, and the cleaned pollutants shall be disposed of in a centralized manner according to medical wastes.
The secretion of the case should be collected in a special container, and soaked and disinfected for 2 hours with chlorine-containing disinfectant with available chlorine of 20000mg/L according to the ratio of substance to medicine of 1:2.
After removing pollutants, the polluted environment and the surface of objects should be disinfected. Containers containing pollutants can be soaked in chlorine-containing disinfectant solution with available chlorine of 5000mg/L for 30 minutes, and then cleaned.
6. Floor and wall.
When there are pollutants visible to the naked eye, the pollutants should be completely removed before disinfection. When there are no pollutants visible to the naked eye, chlorine-containing disinfectant with available chlorine of 1000mg/L or chlorine dioxide disinfectant of 500mg/L can be wiped or sprayed for disinfection; Non-corrosion-resistant floors and walls can also be sprayed or wiped with 2000mg/L quaternary ammonium salt disinfectant; Disinfection time is not less than 30 minutes.
7. Object surface.
When there are visible pollutants on the surface of medical facilities and equipment, bed fences, bedside tables, furniture, door handles, sanitary ware and household items, they should be completely removed before disinfection. When there are no pollutants visible to the naked eye, use chlorine-containing disinfectant with available chlorine of 1000mg/L or chlorine dioxide disinfectant with available chlorine of 500mg/L, and spray, wipe or soak the surface of non-corrosive objects with quaternary ammonium salt disinfectant of 2000mg/L, and clean them with water after 30 minutes.
8. Sewage and feces.
Before entering the municipal drainage pipe network, it needs to be disinfected, and the disinfected sewage shall conform to the Discharge Standard of Water Pollutants for Medical Institutions (GB18466-2005).
9. Case domestic garbage.
Case domestic waste is treated as medical waste.
10. Medical waste.
The disposal of medical wastes shall comply with the requirements of the Regulations on the Management of Medical Wastes and the Measures for the Management of Medical Wastes in Medical and Health Institutions. After being packaged in double-layer yellow medical waste collection bags, the medical wastes shall be disposed according to the conventional process.
11. indoor air
If it is necessary to disinfect indoor air after scientific evaluation, disinfectants such as 5000mg/L peracetic acid, 3% hydrogen peroxide and chlorine dioxide (concentration according to product specifications) can be selected to disinfect indoor air by ultra-low volume (aerosol) spraying method at a rate of 20mL/m3. Other disinfection methods that have been proved to be safe and effective can also be used.
Second, matters needing attention
On-site disinfection should ensure that the disinfection products used is legal and effective, and the selected disinfection method is scientific and feasible. During on-site disinfection, qualified and effective personal protective equipment shall be selected according to the on-site conditions and relevant standards, and disinfection shall be carried out in strict accordance with the work plan on the premise of personal protection.
Disinfection implementation units should have on-site disinfection capabilities, and operators should be trained in disinfection, master the basic knowledge of disinfection and personal protection, and be familiar with the use of disinfection equipment and the preparation of disinfectants.
Disinfection records should be made every time disinfection work is carried out, including disinfection object, disinfection area (volume), disinfectant concentration (or disinfection equipment strength), dosage, action time, etc. At the same time, relevant departments and units should do a good job in supervision, management and evaluation of disinfection work.
Annex 6
Personal protection guide for monkeypox
This guide is formulated to strengthen the personal protection of the public, staff related to epidemic situation handling and medical personnel, and to avoid exposure and infection of monkeypox virus.
A, home isolation treatment cases and other related personnel.
(1) Scope of application.
Personal protection for cases (suspected cases and confirmed cases), caregivers or co-residents who are suitable for home isolation treatment.
(2) Requirements for home isolation areas.
1. Rooms with natural ventilation and independent bathrooms should be selected as isolation areas.
2. Special tableware, bedding such as sheets and towels, personal protective equipment such as disinfectants and masks, and electronic equipment such as televisions and tablet computers shall be provided.
3. The toilet should be equipped with a special washing machine, and the floor drain should be sealed.
(3) Requirements for case management.
1. Should be able to take care of themselves.
2. Temperature measurement and symptom monitoring should be done every day to avoid sharing personal belongings with others.
3. Avoid sexual contact with others, avoid direct contact with people with low immunity, children, the elderly, pregnant women and other people, avoid contact with animals such as pets, and avoid donating blood.
4. When going out to see a doctor, you should wear a medical surgical mask and long trousers to ensure that all damaged skin is covered, avoid close contact with others, and avoid taking public transportation.
(4) Requirements of caregivers.
1. Temperature measurement and symptom monitoring should be done every day.
2. Try to avoid entering the isolation area. If you need to enter the isolation area, you should wear a medical surgical mask and disposable gloves, and keep a distance of at least 1 meter from the case. After leaving the isolation area, hand hygiene should be strengthened, and the masks and gloves taken off should be disinfected and discarded.
3. In the process of handling and cleaning the sheets, clothes and garbage of home isolation treatment cases, jitter should be avoided. Mop the floor with a wet mop to avoid dry sweeping. Clean the surface of household articles with a wet rag, and the carpet should be cleaned with steam to avoid using a vacuum cleaner.
4. Tableware, sheets, towels and clothes for home isolation treatment cases should be washed and disinfected separately, and disinfection methods such as thermal disinfection, chlorine-containing disinfectant or quaternary ammonium salt disinfectant soaking can be selected.
(5) Emergency handling.
1. Caregivers or co-residents who have any symptoms or discomforts should go to the designated medical institutions in time and report the suspicious contact history on their own initiative.
2. Disinfect the articles in contact with them and the areas where they are active in combination with the risk assessment results.
Second, the epidemic disposal related staff
(1) Scope of application.
It is suitable for epidemiological investigation and personal protection of environmental cleaning and disinfection personnel during the epidemic of monkeypox.
(2) Protection requirements for epidemiological investigators.
1. Personal protective equipment. Disposable latex gloves, medical surgical masks, disposable isolation gown, etc.
2. Personal protection requirements. Standardize wearing masks, strengthen hand hygiene, and keep a distance of at least 1 meter from the person being investigated.
3. Waste management. After the investigation, the temporary storage, treatment and disposal of abandoned personal protective equipment shall be carried out in accordance with the Regulations on the Management of Medical Wastes.
4. Emergency treatment. If the mask falls off or directly touches the skin or secretion of the case during the investigation, the risk assessment should be carried out in combination with the clinical diagnosis results of the investigated personnel, the tightness of the space, the time and distance of contact, and corresponding treatment measures should be taken in combination with the risk assessment results.
(3) Protection requirements for environmental cleaning and disinfection personnel.
1. Personal protective equipment. Disposable latex gloves, medical surgical masks, disposable isolation gown, waterproof boot covers, etc.
2. Personal protection requirements. Standardize wearing masks, strengthen hand hygiene, and minimize direct contact with sterilized items.
3. Waste management. After cleaning and disinfection, the temporary storage, treatment and disposal of abandoned personal protective equipment shall be implemented in accordance with the Regulations on the Management of Medical Wastes.
4. Emergency treatment. In case of mask falling off, skin injury or direct contact with excrement and blood during cleaning and disinfection, risk assessment should be made in combination with the type of the cleaned and disinfected articles, the contact time and the tightness of the space, and corresponding disposal measures should be taken in combination with the risk assessment results.
Third, the personal protection of medical personnel
(1) Scope of application.
It is suitable for the protection of medical staff and their working environment during the epidemic of monkeypox.
(2) Basic requirements.
1. Personal protective equipment requirements. Medical personnel shall carry out standard prevention, adopt isolation and prevention measures for diseases transmitted by contact and droplets, and wear disposable latex gloves, masks of KN95/N95 and above, protective screens or goggles, disposable isolation gown, etc.
2. Environmental protection requirements. The cleaning and disinfection of hospital environment shall meet the requirements of Annex 5. Activities such as dry dust removal, cleaning or vacuuming should be avoided. Wet cleaning method is preferred.
3. Waste management. Temporary storage, treatment and disposal of personal protective equipment and case dressings shall be carried out in accordance with the Regulations on Management of Medical Wastes.
Annex 7
Technical guide for laboratory detection of monkeypox virus
In order to guide the disease control departments at all levels and other relevant institutions to standardize the laboratory detection of monkeypox virus and quickly and accurately identify the confirmed cases of monkeypox, this guide is formulated. This guide mainly introduces specimen collection, detection method of monkeypox virus nucleic acid by fluorescence quantitative PCR, biological safety requirements and so on.
First, the detection object
(a) confirmed cases and suspected cases of monkeypox;
(2) Close contacts;
(3) Animals infected or suspected of being infected with monkeypox virus;
(4) Environment or other biological materials.
Second, the basic requirements of technical personnel
(1) Sampling personnel. Technical personnel engaged in the collection of monkeypox virus nucleic acid detection samples shall undergo biosafety training, and can only engage in sampling work after passing the training. Sampling personnel should be familiar with the types and methods of collecting specimens, master the operation process and matters needing attention of specimen collection, and record the specimen information to ensure that the specimen quality meets the requirements and the specimen and related information can be traced back.
1. Personal protective equipment requirements for sampling personnel: masks of KN95/N95 and above, protective screen or goggles, disposable isolation gown, disposable latex gloves (wear two layers as far as possible) and boot covers; If you come into contact with the blood, body fluids, secretions or excreta of the case, you should change your gloves in time. Sewage sampling personnel can appropriately reduce the protection level according to the actual work needs.
2. The specimens of hospitalized cases are collected by the medical staff of the hospital where they are located. According to the needs of laboratory testing, they can be sampled many times in combination with the course of disease.
3. Specimens of close contacts are collected by local disease control institutions or professionals of medical institutions.
4. Animals infected with or suspected of being infected with monkeypox virus shall be collected by professional sampling personnel of the local disease control agency in coordination with the animal epidemic control department.
5. Samples of environmental or other biological materials shall be collected by relevant professional sampling personnel.
(2) testing personnel. Laboratory testing technicians should have a college degree or above in related majors or have intermediate or above professional and technical qualifications, have more than 2 years of laboratory work experience, have received training in nucleic acid testing, and can only engage in testing after passing the training. The number of staff in the laboratory should be appropriate to the testing items and specimen quantity, so as to ensure that the laboratory testing and reporting results can be carried out in a timely, skilled and accurate manner.
III. Specimen Collection, Preservation and Transportation
(1) Specimen collection types.
1. The preferred specimen is the skin (mucosa) lesion site specimen, including the lesion surface swab, pox blister fluid or pox blister exudate swab, pox scab or pox scab swab, etc.
2. Respiratory tract specimens, such as oropharyngeal swabs, can be used to detect acute cases and are also the most commonly used specimens for close contacts.
3. EDTA anticoagulant samples can be collected for nucleic acid detection in the acute stage of onset.
4. Collect two serum samples for antibody detection within 7 days (acute phase) and 3-4 weeks (recovery period) after onset.
5. rectal swab, urine, semen, saliva and other specimens are only used for research and collected according to work needs.
6. Samples of sewage or other environmental biological materials shall be collected according to actual work needs.
(2) Specimen collection requirements.
Sterile polyester fiber, nylon or similar material swab should be used when collecting skin (mucosa) lesions, and cotton swab should be avoided. 75% ethanol and other disinfectants should be avoided to clean the diseased parts before collecting specimens of suspected cases. More than two swabs should be collected as far as possible for each type of skin (mucosal) lesions, and 2-3 specimens of different parts of the body or different appearances should be collected at the same time for each case. When collecting skin (mucosa) lesions, appropriate force should be applied. Different swab specimens such as skin (mucosa) lesions, acne scabs or secretions should be placed in different sampling tubes. When virus separation is carried out, dry swab specimens (without sampling solution) should be collected or preserved with non-inactivated virus sampling solution. According to the qualification of laboratory activities, it is determined to use non-inactivated or inactivated sampling liquid to collect samples.
(3) Specimen collection method.
1. Specimens of skin (mucosa) lesions such as macula, papule, blister or pustule: Hold the tail of the sampling swab with one hand, and keep a distance of more than one inch from the head of the swab. When sampling, press down the swab with proper force, wipe it back and forth at least 2-3 times, and then wipe it again with the other side of the swab for 2-3 times. If the blain is broken during wiping, make sure to collect the blain liquid. After sampling, put the swab in a sterile sampling tube (which may or may not contain virus sampling liquid), break the swab head, remove the tail of the swab, cover the tube cover, wipe the sterilized sampling tube with a disinfectant paper towel, and seal the tube cover with a sealing film before storing or sending it for inspection.
2. Skin (mucous membrane) specimens with acne scabs or blisters: Before sampling, it should be ensured that such specimens can be detected in the laboratory. Use sterile tweezers or other blunt instruments to clamp all acne scabs or scab skin with an area of at least 4mm×4mm, put them in a dry and sterile sampling tube, and cover the affected area with a band-aid after sampling.
3. Oropharyngeal swab specimen: The head of the person to be collected leans slightly, the mouth is wide open, and the tonsils on both sides are exposed. The swab crosses the base of the tongue, and the tonsils on both sides of the person to be collected are slightly wiped back and forth for at least 3 times, and then the swab head is wiped up and down the posterior pharyngeal wall for at least 3 times. Immerse the swab head in a tube containing 2-3mL virus preservation solution or put it in a sterile tube containing no liquid (dry swab), discard the tail and tighten the tube cover.
4. Blood samples: Try to collect blood samples in the acute phase (within 7 days of onset). It is recommended to collect 5mL whole blood by using a vacuum blood collection tube containing EDTA anticoagulant, which can be used for detection, or stand at room temperature for 30min, centrifuge at 1500-2000rpm for 10min, and collect plasma in a sterile tube for detection.
5. Serum sample: Collect 5mL of blood sample with vacuum negative pressure blood collection tube, stand at room temperature for 30min, centrifuge at 1500-2000rpm for 10min, and collect serum in sterile screw plastic tube. The first serum should be collected as soon as possible (preferably within 7 days after the onset), and the second serum should be collected in the 3-4 weeks after the onset. After collecting 5mL of blood samples, let it stand at room temperature for 30 minutes, centrifuge at 1500-2000rpm for 10 minutes, and collect the serum in a sterile screw plastic tube for the detection of monkeypox antibodies.
6. Other specimens: collected according to the design requirements.
(4) specimen preservation.
Specimens should be refrigerated (2-8℃) or frozen (-20℃ or below) within 1 hour after collection, and tested as soon as possible. Specimens that can be detected within 1 week can be stored at 4℃; Specimens that cannot be detected within 1 week can be stored at -20℃ in the short term and at -70℃ or below in the long term. The whole blood is refrigerated (2-8℃) before plasma separation, and the separated plasma is stored at -20℃ or below. A special library or special counter should be set up to store specimens separately to avoid repeated freezing and thawing of specimens.
Monkeypox virus and its related specimens should be managed by special personnel, and the source, number and quantity of the virus and specimens should be accurately recorded. For specific requirements, please refer to the General Rules for the Description of Preservation Data of Pathogenic Microorganisms (Viruses) (T/CPMA 011-2020). Effective measures should be taken to ensure the safety of viruses and specimens, and prevent incidents such as misuse, malicious use, theft, robbery, loss and disclosure.
(5) Specimen inspection.
Samples should be sent to the laboratory at low temperature (ice bag or dry ice) as soon as possible after collection. If it is necessary to transport samples for a long distance, dry ice freezing transportation should be used for preservation.
1. Specimens for inspection: The case specimens shall be initially detected by the provincial and below CDC, and the first monkey pox positive specimen in each province shall be sent to the Institute of Virology of China CDC for review. At least one set of samples (skin or mucosal lesion site samples, oropharyngeal swab samples and acute and recovery serum samples) shall be collected from each positive case and sent to the Institute of Virology, China CDC for testing. The provincial CDC shall formulate the process of sample inspection and review in the province according to the actual situation.
2. Transport of pathogens and specimens:
(1) Domestic transportation. The transportation and packaging classification of monkeypox virus or other potentially infectious biological materials belongs to Class A, and the corresponding UN number is UN2814. The packaging conforms to the classification and packaging requirements of PI602 in the ICAO document Doc9284 "Technical Rules for Safe Aviation Transportation of Dangerous Goods". For those transported by other means, please refer to the above standard packaging. The transportation of monkeypox virus or other potentially infectious materials shall be carried out in accordance with the Regulations on the Transportation Management of Highly Pathogenic Microorganisms (Viruses) that can infect humans (Order No.45 of the former Ministry of Health). Environmental samples such as sewage are temporarily implemented according to the transportation standard of ordinary biological samples.
(2) International transportation. When the monkeypox virus strains or samples are transported internationally, the packaging should be standardized, the relevant procedures should be handled in accordance with the Provisions on the Administration of Health and Quarantine of Entry-Exit Special Articles, and the relevant national and international requirements should be met.
Four, monkeypox virus nucleic acid detection requirements and process
(a) laboratory qualification requirements.
Laboratories that carry out nucleic acid detection of monkeypox virus shall comply with the relevant provisions of the Regulations on Biosafety Management of Pathogenic Microbiological Laboratories (Order No.424 of the State Council) or the Measures for the Administration of Clinical Gene Amplification Laboratory in Medical Institutions (No.194 of Wei Ban Yi Zheng Fa [2010]), and have the conditions of BSL-2 laboratories and above registered by the municipal health department with districts, and record the experimental activities related to monkeypox virus. Independent medical laboratory should also meet the requirements of Basic Standards for Medical Laboratory (Trial), Management Standard for Medical Laboratory (Trial) and so on.
Laboratories involved in virus amplification, use and other experimental operations such as isolation, culture and neutralization of monkeypox virus should meet the requirements of BSL-3 laboratories and above approved by the National Health and Wellness Commission, and obtain the approval of monkeypox virus experimental activities. The isolated monkeypox virus should be sent to the National Pathogenic Microbiology Preservation Center/National Pathogenic Microbiology Resource Library for virus sub-storage.
(2) Laboratory biosafety requirements.
According to the List of Pathogenic Microorganisms Infected by Human Beings published and implemented in 2006, the biological hazards of monkeypox virus are classified into the first category, which is a highly pathogenic virus. According to the requirements of the Catalogue, the isolation and cultivation of monkeypox virus and other experimental operations involving virus amplification and use should be carried out in the biosafety cabinets of BSL-3 and above laboratories; Inactivation of monkeypox case samples collected by non-inactivated sampling solution was carried out in BSL-3 laboratory. After the sample is inactivated, the extraction and detection of monkeypox virus DNA can be carried out in BSL-2 and above laboratories or in special areas or rooms for PCR detection. If the Catalogue is updated, the laboratory biosafety requirements for monkeypox virus operation should be implemented according to the latest Catalogue. Inactivation of sewage samples refers to common biological samples.
(3) Requirements for laboratory zoning.
In principle, the laboratory for detecting monkeypox virus nucleic acid should set up the following areas: reagent storage and preparation area, specimen preparation area, amplification and product analysis area. The three areas should be completely independent of each other in physical space, and the air should circulate directionally. The functions of each district are:
1. Reagent storage and preparation area: preparation of storage reagents, sub-packaging of reagents and preparation of amplification reaction mixture, as well as storage and preparation of consumables such as centrifuge tubes and suction heads.
2. Specimen preparation area: the transfer barrel is opened, the specimen is inactivated, and the nucleic acid is extracted and added to the amplification reaction tube.
3. Amplification and product analysis area: nucleic acid amplification and product analysis.
According to the function of the instrument used, the areas can be merged appropriately. If an automatic analyzer integrating sample processing, nucleic acid extraction and amplification detection is adopted, the sample preparation area, amplification area and product analysis area can be merged.
(4) Main instruments and equipment.
The laboratory should be equipped with instruments and equipment suitable for carrying out inspection items, including: secondary biosafety cabinet, high-speed desktop centrifuge, dry bath thermostat, fluorescence quantitative PCR instrument, timer and pipette.
(5) Laboratory monkeypox virus nucleic acid detection process.
After the laboratory receives the specimen, it carries out reagent preparation, specimen pretreatment, nucleic acid extraction, nucleic acid amplification, result analysis and report according to standard operating procedures. The laboratory shall establish a re-examination process for suspicious specimens and positive specimens.
1. Reagents and materials.
(1) Specimens: including specimens of diseased surface swab, pox blister fluid or pox blister exudate swab, pox scab or pox scab swab, throat swab, whole blood or plasma, etc.
(2) nucleic acid extraction kit (genomic DNA extraction kit): tissue genomic DNA extraction kit or blood/cell/tissue genomic DNA extraction kit.
(3) nucleic acid detection reagent:
① reagent: DNA polymerase or pre-mixed PCR Master Mix.
② Primers and probes for detection of monkeypox virus:
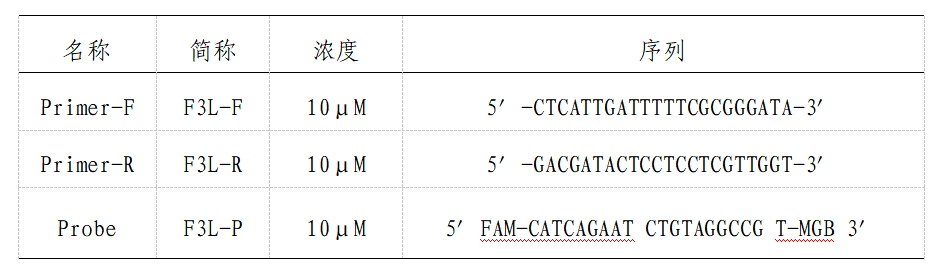
③ Positive control: plasmid covering the detection target sequence.
(4) sterilizing deionized water and anhydrous ethanol
(5) disinfectant
①75% ethanol: used for routine disinfection of hands and surfaces, and valid for 1 week after opening.
(2) Chlorine-containing disinfectant: the disinfectant containing 1000mg/L of available chlorine is used for routine disinfection of the surface of objects, and the disinfectant containing 5000mg/L of available chlorine is used for emergency treatment when infectious materials spill.
(6) Consumables: including suction head with filter element, centrifugal tube with spiral mouth, centrifugal tube without spiral mouth, crushing tube containing zirconium beads, PCR reaction plate, transparent sealing film or PCR reaction tube and transparent cover.
(7)BSL-2 Personal protective equipment: including masks of KN95/N95 and above, disposable isolation gown, protective goggles or face screen, disposable hats, shoe covers, boot covers and gloves.
2. Specimen reception before the experiment.
(1) Check the number, name, sex, age and test items of the tested specimen;
(2) If there is any abnormality in the state of the specimen to be tested, please indicate it;
(3) The specimen to be tested can be stored at -70℃ for a long time and at -20℃ for a short time to avoid repeated freezing and thawing.
3. Steps and precautions for nucleic acid detection.
(1) preparation of viral nucleic acid (DNA)
The operation method is as follows according to the corresponding instructions of the DNA extraction kit:
① Preparation of extraction reagent: open the kit for the first time, add anhydrous ethanol to the rinse solution before use, and add the volume reference bottle to label it. All reagents should be balanced to room temperature before use; All centrifugation steps should be carried out at room temperature.
② Processing samples:
A. pox blister fluid: dry swab specimens need to be resuspended with PBS or DMEM containing PS in an appropriate volume for detection. Take 100μ L sample, add 80μ L buffer solution, the total amount is 180μ L; The specimen volume is less than 100μ When l, make up the total volume to 180&mu with buffer solution; L;
B. Lesion rash or acne scab: Take one scab skin according to the mass/volume (1mg/50μ L) adding corresponding volume of PBS containing PS, grinding or homogenizing, and taking 80μ L, and then add 100μ L buffer;
C throat swab and other swabs: take 200&mu from the sampling solution; L specimen and dry swab specimen can be resuspended with 3mL PBS or DMEM containing PS, and 200&mu is taken after mixing; L;
D. Whole blood or serum: directly take 200μ L specimen.
③ adding 20μ L protease k solution, mixed well, the solution will become clear. If the sample is a diseased rash or other tissues, add protease K and mix well, then leave it at 56℃ until the tissues are dissolved, and then proceed to the next step.
④ adding 200μ L crack the buffer solution, mix it thoroughly, let it stand at 70℃ for 10 minutes, or until the solution becomes clear, and centrifuge briefly to remove the water droplets on the inner wall of the tube cover.
It should be noted that white flocculent precipitate may appear after adding cracking buffer, and it will disappear after standing at 70℃. If the solution is not clear, it means that the cell lysis is not complete, which may lead to a small amount of extracted DNA or impure DNA.
⑤ Add 200μ L anhydrous ethanol, fully mixed, flocculent precipitation may occur at this time, and briefly centrifuge to remove water droplets on the inner wall of the pipe cover.
⑥ Add the solution and flocculent precipitate obtained in the previous step into an adsorption column (the adsorption column is put into a waste liquid collection tube), centrifuge at 8000rpm for 1 minute, and discard the waste liquid.
⑦ Add 500μ L rinse buffer 1 (check whether absolute ethanol has been added before use), centrifuge at 8000rpm for 1 minute, and discard the waste liquid.
⑧ Add 500μ L rinse buffer 2 (check whether absolute ethanol has been added before use), centrifuge at the maximum speed of 13000rpm for 3 minutes, and discard the waste liquid.
Pet-name ruby put the adsorption column back into the waste liquid collection tube, centrifuge at the maximum speed of 13000rpm for 1 minute, and try to remove the rinsing liquid.
Attending to transfer the adsorption column into a clean centrifuge tube (it needs to be prepared by itself, which is not provided in the kit), and add 50μ L Elute the buffer or sterilized deionized water, stand at room temperature for 2-5 minutes, and centrifuge at 8000rpm for 1 minute. Collect the filtrate, mark it, and store it at 4℃ or -20℃ (short term) for later use, and at -70℃ for long term.
(2) Nucleic acid detection: real-time fluorescence quantitative PCR(qPCR) was used to detect the nucleic acid of monkeypox virus (conducted in PCR laboratory).
① Preparation of reaction system: 20&mu per hole; L, add 5μ L sample DNA, 25&mu in total; L; Every PCR reaction, in addition to the detection of samples, should add no DNA control (water instead of DNA), positive control; All samples, including controls, should be provided with multiple holes.
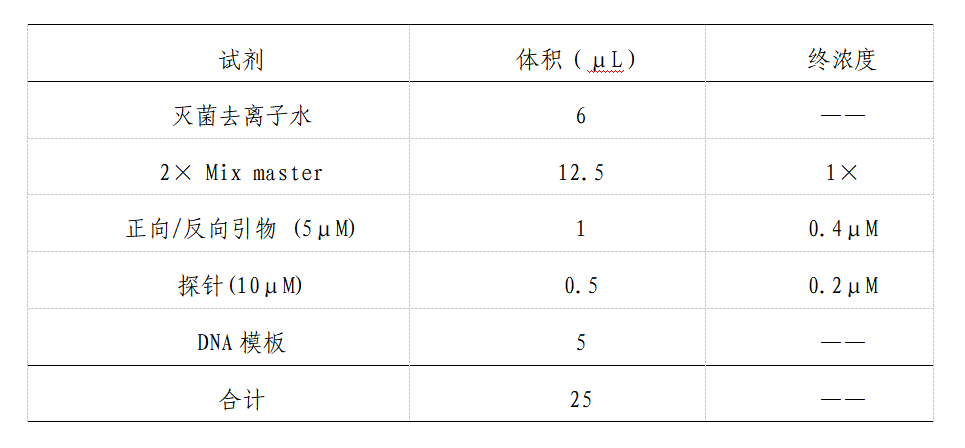
② Sample addition: add 5uL of nucleic acid or control into each reaction tube, cover the tube tightly or seal the transparent film, and put it on the fluorescent quantitative PCR detector.
③ amplification condition setting:
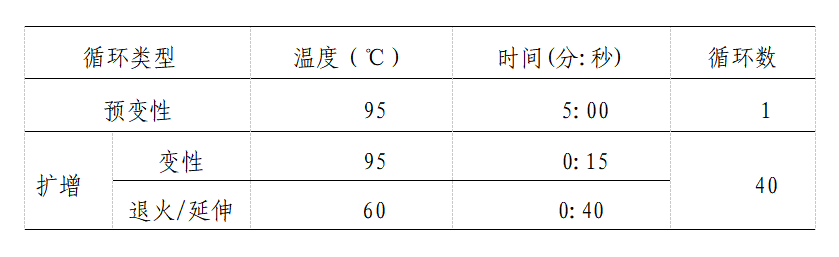
④ Selection of instrument detection channel: use fluorescence quantitative PCR detector, select Fam fluorescence signal detection channel, and set the collection at 60℃. Refer to the instruction manual of each instrument for the specific setting method.
⑤ Threshold setting for result analysis: When using the fluorescence quantitative PCR detector to analyze the results, the baseline is 3-10 or 6-15 cycles of fluorescence signals. The threshold setting principle is that the threshold line just exceeds the highest point of the normal negative control amplification curve, and the threshold can also be adjusted according to the noise of the instrument.
(3) Judgment of nucleic acid detection results
① Quality control of ①Real-time PCR reaction system: the reaction results should meet the following two conditions at the same time, otherwise the test results will be invalid, and the test should be carried out again. The negative control was negative without amplification. No negative results were found in the positive control.
② Result determination:
A. negative: double-hole Ct value > 37, or no Ct value;
B. gray area: the Ct value of a hole is > 37;
C. positive: double-hole Ct value < 37.
All positive and gray samples should be repeatedly tested or confirmed by sequence analysis. It should be noted that when the specimen is only throat swab or serum or plasma, and the test result is negative, the negative diagnosis should be made carefully in combination with clinical symptoms.
(4) Form record
Do a good job in the original record of detecting monkeypox virus nucleic acid by fluorescence quantitative real-time PCR.
5. Sequencing the whole genome of monkeypox virus
1. Selection principle of sequencing samples. The first or early cases in the local epidemic, the key cases related to the early cases, the local cases with unknown sources of infection, and the positive specimens of imported cases. The Ct value of the above samples was detected by nucleic acid fluorescence quantitative PCR ≤ Sequencing was performed at 32: 00 (except for key samples).
2. Sequencing requirements. Determine the institutions to carry out the whole genome sequencing of monkeypox virus by province. It is suggested that amplicon technique be used to sequence the whole genome of monkeypox virus. The sequencing data can be used for subsequent bioinformatics analysis only after passing the quality control. The coverage depth of the second-generation sequencing platform should be not less than 10×, the coverage depth of the third-generation sequencing platform should be not less than 50×, and the coverage of whole genome sequencing should be not less than 98%. The comparison and analysis of data recommended reference monkeypox genome NC_063383.1.
Each province should establish the genome database of imported and local cases of monkeypox virus, which should have the ability of sequence comparison and analysis. Provinces with sequencing conditions should carry out sequencing work within 48 hours after receiving samples. For key samples, the laboratory is required to provide a sequencing result report within 1 week after receiving samples. All original sequencing data (generally in fastq format), assembly sequence (generally in fasta format) and specimen sequencing result report (see Annex 7-2) should be submitted to the Institute of Virology, China CDC for sequence summary and analysis within 48 hours after obtaining the sequence. The Institute of Virology shall timely feed back the sequence analysis results to the provinces, and summarize the national monkeypox virus sequences and report the analysis results to the National Bureau of Disease Control and Prevention in time.
3. Molecular typing. NextClade (https://clades.nextstrain.org), an online analysis tool, is recommended for molecular typing of mutant strains.
Attachment:
7-1 Inspection Form for Monkeypox Virus Detection Specimens
7-2 Report on Sequence Determination Results of Monkeypox Virus Specimens